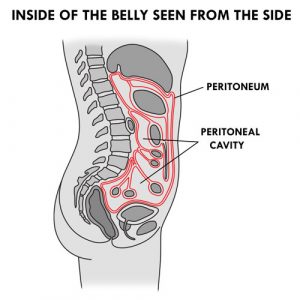
The peritoneum is the cavity inside of the abdomen that holds internal organs (eg, stomach, intestines, liver) and helps to hold these organs in place. The lining of the peritoneum is called the peritoneal membrane. The space between the organs is called the peritoneal cavity.
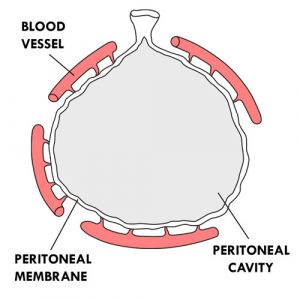
The peritoneum can be compared to an inflatable balloon. The interior of the balloon corresponds to the peritoneal cavity and the walls of the balloon to the peritoneal membrane. The “balloon” (peritoneum) is deformed to go around the internal organs. The peritoneal membrane contains millions of tiny blood vessels.
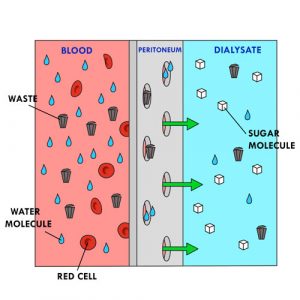
The peritoneal membrane has several characteristics that allow it to act as a filter:
it is porous (filled with small microscopic holes),
it is semi-permeable (lets water through but not large particles such as red blood cells),
it is bi-directional (liquids can pass on both sides),
it has a large surface area (0.5 to 2 square meters, depending on the child’s body surface).
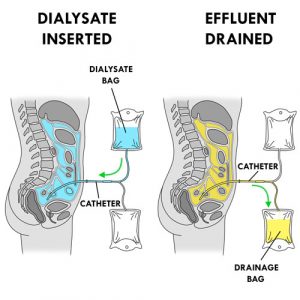
The operation of peritoneal dialysis is simple. A special solution (dialysate or dialysis solution) is injected through a catheter into the peritoneal cavity. The blood is separated from the dialysate by the peritoneal membrane. The blood, containing waste products, excess water and mineral salts, comes into contact with the dialysate, which contains no waste products. The water and waste products pass through the peritoneal membrane from the blood to the dialysate. The dialysate absorbs the waste products and the surplus of mineral salts and water from the blood to the filtering capacity of the peritoneum. The good elements remain in the blood (eg,, red blood cells). The soiled dialysate (effluent or drainage fluid), filled with waste, is then drained through the same catheter outside the body into a drainage bag before being discarded. The effluent is yellow in color like urine.
Peritoneal dialysis is done through exchanges. Each exchange (or cycle) consists of three phases: 1. drainage phase: exit of the soiled dialysate (effluent) from the peritoneal cavity to the outside; 2. infusion phase: entry of the new dialysate into the peritoneal cavity; 3. dwell (or contact) phase: period of time during which the dialysate remains in the peritoneal cavity and the cleaning of the blood takes place; the waste products and the surplus of water and mineral salts of the blood pass through the peritoneal membrane and go into the dialysate, which becomes progressively soiled.
The volume of dialysate introduced during the infusion phase depends on the child’s weight or body surface area. Depending on the child’s specific needs, several exchanges must be performed to remove some of the waste products from the blood and make the child feel better. This treatment is not painful.
The filtration of blood by the peritoneum is done thanks to two natural processes which can last from several minutes to a few hours:
diffusion: movement of waste through a semi-permeable membrane (eg, the peritoneum). The waste passes from a medium where it is more concentrated (eg, blood) to a medium where it is less concentrated (eg, the dialysate) until there is a balance on both sides of the membrane.
osmosis: movement of water molecules through a semi-permeable membrane (eg, the peritoneum) from a solution where there is more water (eg, blood) to a solution where there is less (eg, the dialysate), until a balance is reached. The water crosses from a less concentrated medium to a more concentrated medium.
The dialysate is a sterile solution containing sugar (eg, glucose, dextrose), mineral salts (eg, sodium, calcium, magnesium, chlorine) and a buffer solution containing lactate, bicarbonate or lactate-bicarbonate) at an acidic (5.5) or neutral (or physiological) pH (7.4).
It is the large sugar molecules in the dialysate that draw excess water into the bloodstream by osmosis. The concentration of sugar in the dialysate varies according to the amount of water to be removed. The higher the sugar concentration, the more water molecules in the blood are drawn into the dialysate. On the contrary, the lower the sugar concentration, the less water molecules in the blood pass through into the dialysate.
This process is called ultrafiltration (UF). It is also referred to as the “balance” which represents the difference between the dialysate entering the abdomen and the fluid leaving it.
At the end of a dialysis session, a positive balance refers to the dialysate retained by the child. For example, a 500 ml infusion with a 400 ml drainage corresponds to a positive balance of + 100 ml. The child retained 100 ml of the 500 ml administered. A negative balance refers to the dialysate and excess fluid removed from the child. For example, a 500 ml infusion with a 700 ml drainage corresponds to a negative balance of – 200 ml. The child has therefore eliminated 200 ml more than the amount of dialysate infused.
The sugar concentration of the dialysate is indicated by the color of the pull ring on the bag:
white: 0.5%
yellow: 1.36% or 1.5%
green: 2.27% or 2.5%
orange: 3.86% or 4.25%
The bag with the purple pull ring contains 7.5% icodextrin which is glucose polymer.
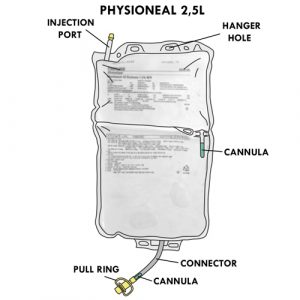
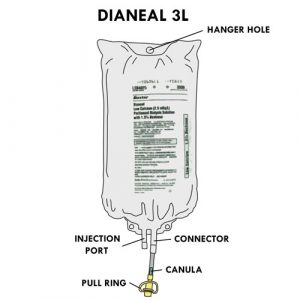
Each dialysate bag has:
an injection port: allows you to add medication to the solution,
a hanger hole: to hang the bag,
a connector: to connect the bag to a tubing for treatment,
a cannula (or cone) in the stem of the connector: breaking the cannula allows the solution to flow out,
a pull ring: to protect the end of the connector; its shape facilitates its removal to connect the connector to a line (or tubing) for treatment.
There are several types of dialysate, with varying concentrations and sizes. Here are the ones that are most often used for children at home:
SORT OF DIALYSATES
(Source: Baxter International Inc.)
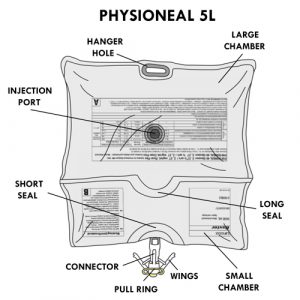
Physioneal™
Contains glucose/dextrose in concentrations of 1.36%, 2.27% or 3.86%, sodium, calcium, magnesium, chloride, lactate and bicarbonate.
Available in 2.5 and 5 liter bags.
Has a neutral pH (7.4).
Has two chambers (or compartments) containing different solutions.
Specifics for the 2.5 liter format:
Has a cannula between the two chambers, to be broken to mix the solutions.
Specifics for the 5 liter format:
Has a small and a large chamber.
The injection port is located at the back of the large chamber.
Has two seals:
a long seal separates the two chambers; the opening of the long seal allows mixing of solutions.
a short seal separates the small chamber from the connector; the opening of the short seal will allow the solution to flow into the connector.
The connector has wings: closing the wings advances the connector cannula to puncture the bag and allow the solution to flow into the tubing for treatment.
Dianeal™
Contains glucose in concentrations of 0.5%, 1.5%, 2.5% or 4.25%, sodium, calcium, magnesium, chloride and lactate.
Available in 2, 3 or 5 liter bags.
Has an acidic pH (5.5).
Extraneal™
Contains icodextrin (a molecule larger than glucose) in a concentration of 7.5% as well as sodium, calcium and magnesium, chloride and lactate.
Available in 2.5 liter bags only.
Has an acidic pH (5.5).
Used once a day for a long dwell time.
The amount of waste and water removed during a dialysis session depends on the type and concentration of the solution, the duration of the dwell phase and the filtration capacity (permeability) of the peritoneal membrane. Sometimes the healthcare team will recommend a change in the type of dialysate during the course of treatment because of certain signs of dehydration or fluid overload present in the the child (eg, rapid weight change, blood pressure too high or too low, presence or absence of swelling, etc.). Do not hesitate to discuss this with your child’s healthcare team.
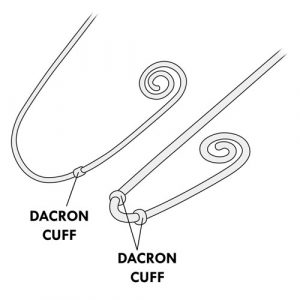
Peritoneal dialysis requires the installation of a small flexible tube, the peritoneal catheter, to allow the dialysate to enter and exit the peritoneal cavity. This catheter is installed surgically in the abdomen, on the right or left side. Different types of catheters can be used.
The catheter has an external and an internal part. The catheter has one or two dacron cuffs in the internal part, allowing it to be stabilized under the skin and inside the peritoneal cavity. These cuffs are not visible from the outside.
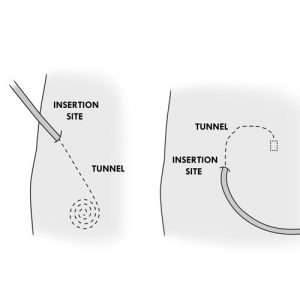
The catheter insertion site (or entry site or catheter site) is the skin around the catheter. The bump or line you feel under the skin a few inches from the catheter insertion site is the beginning of the inner part and is called a “tunnel”. The tunnel is the path of the catheter under the skin, from the insertion site to the peritoneal cavity.
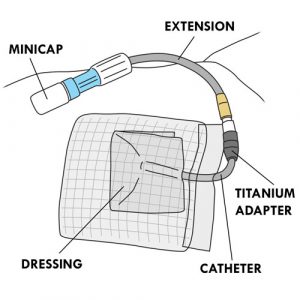
The child keeps the catheter in place as long as he or she requires peritoneal dialysis, for weeks, months or years. The catheter is connected to a titanium adapter, which in turn is connected to an extension (or transfer line). This extension is protected by a MiniCap disconnect cap between dialysis sessions. The catheter insertion site is covered with a dressing.
There are two methods of peritoneal dialysis. Each has its advantages and disadvantages. With your help, your healthcare team will identify the one that best suits your child’s needs.
METHODS OF PERITONEAL DIALYSIS (PD)
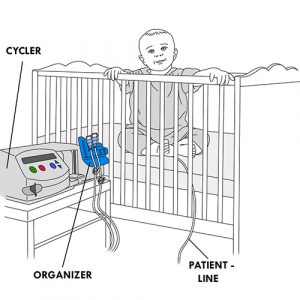
Automated PD (APD)
Automated method using a device (cycler) with constant or no presence of dialysate in the peritoneal cavity.
It consists of approximately four to ten short exchanges at night, according to a pre-established program in the cycler. Daytime exchanges may also be added, depending on the child’s needs.
The dialysate is injected and drained from the peritoneal cavity automatically by the cycler.
This type of peritoneal dialysis is the most frequently used at home for children.
Several types of programming are possible. The most frequently used are:
Continuous cyclic PD (CCPD): In addition to the nighttime exchanges, a longer exchange during the day is added. The cycler is disconnected in the morning upon awakening; dialysate remains in the peritoneal cavity during the day. In the evening, at bedtime, the effluent is drained after connection to the cycler for the night.
Intermittent PD (IPD): Drainage is performed in the morning. The peritoneal cavity remains empty during the day.
Continuous Ambulatory PD (CAPD) or Manual PD
Manual method with constant presence of dialysate in the peritoneal cavity.
Usually consists of four exchanges per day, at regular intervals: morning, noon, late afternoon and at bedtime. The dwell phase is longer at night.
The dialysate enters and leaves the peritoneal cavity by gravity.
This type of dialysis is not very common at home in children. It is mainly used in emergencies when the cycler is not working.
The equipment required for automated peritoneal dialysis includes several accessories:
AUTOMATED PERITONEAL DIALYSIS (PD) EQUIPMENT
(Source: Baxter International Inc.)
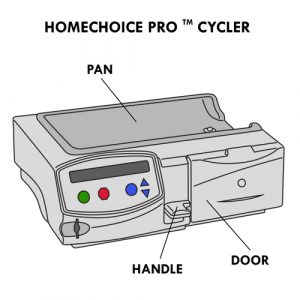
Cycler
There are different models of cyclers (eg, HomeChoice, HomeChoice Pro MC).
Some models allow the use of a memory card to record data.
The handle of the cycler locks/unlocks the compartment where the APD cassette is installed.
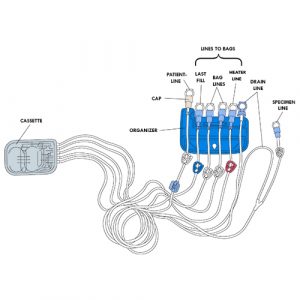
Cycler set with cassette or APD set
Contains several parts:
Cassette: has two separate compartments; one is used to measure the amount of dialysate infused and the other the amount of effluent drained.
Organizer: allows the grouping of tubing in a specific order for use.
Lines (or Tubings):
specimen line: is Y-shaped with the drain line; is used to connect the specimen bag if needed; has a white clamp.
drain line: installed at the far right of the organizer; used to connect the drain bag; does not have a clamp.
heater line: used to connect the bag placed on the heater (empty or full bag); has a red clamp.
bag lines (orsupply lines): are used to connect the dialysate bags for the duration of the treatment, if needed; have white clamps.
last fill line: is used to connect the last dialysate bag for daytime use if the type of solution is different from the solutions used at night; can also be used as an additional bag line if the same dialysate is used for the entire treatment; has a blue clamp.
patient line: installed on the far left side of the organizer; connects the child with the catheter extension for treatment; has a white clamp.
(Click to see larger image)
The end of each line is protected by a protective cap.
The set model used for peritoneal dialysis is specific to children. However, when the volume of dialysate to be injected is ≥ 1000 ml, your healthcare team may suggest that you use the adult model.
The patient line tip is different between the two models:
the patient line tip of the pediatric (child) set fully covers the catheter extension tip when connected;
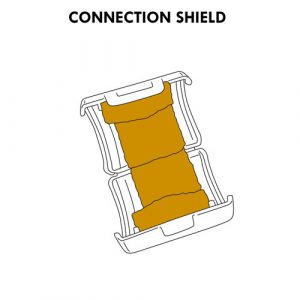
the patient line tip of the adult set only partially covers the end of the catheter extension when connected; some healthcare teams recommend installing a connection shield with povidone-iodine to protect the exposed portion of the extension.
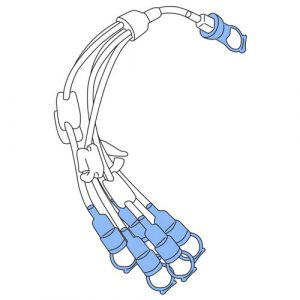
5-Prong manifold set
Allows connection of additional dialysate bags if the 2 bag lines are not sufficient.
Each line has a clamp and its end is protected by a protective cap.
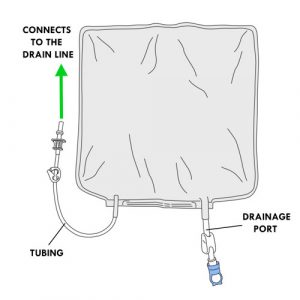
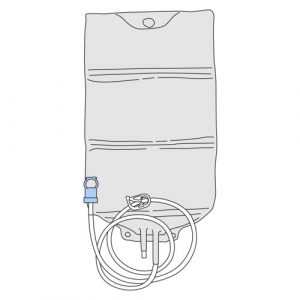
Drainage bag
Collects effluent.
Has a tubing with a perforator protected by a protective cap.
This tubing connects to the drain line of the cycler set with cassette.
Has a drainage port to empty the effluent; its is protected by a protective cap.
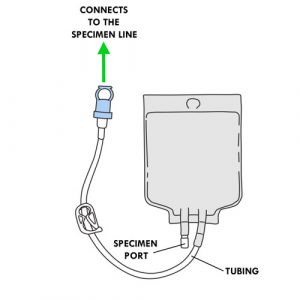
Specimen bag
Collects the effluent specimen.
Has a tubing protected by a protective cap.
This tubing connects to the specimen line of the cycler set with cassette.
Has a specimen port for removing effluent with a syringe.
Empty bag
Installed on the heater as needed.
Is used when the child needs a mixture of dialysates with different concentrations and small volumes infused per cycle.
Dialysis clamp
Allows you to clamp the catheter in case of emergency, disconnection or breakage of the catheter.
Depending on the recommendations of your healthcare team, can also be used to:
secure the closure of the drainage bag tubing through which the effluent is drained;
clamp multi-line extension and bag lines not connected to a dialysate bag during treatment.
Refer to your healthcare team for:
the type of dialysis solutions to use,
the frequency of exchanges to be performed,
the operation of the cycler, if applicable.
Unfortunately, peritoneal dialysis cannot replace everything that healthy kidneys do. The child must therefore follow a specific diet and take vitamins and medication as recommended by the healthcare team.
Your healthcare team is available to supervise the care provided to your child, ensure the proper functioning of equipment and make recommendations to you as needed.
Refer to your healthcare team if the equipment used for your child at home is different from what is described in this section or in the methods of care.
Disclaimer of Liability: By using this site, you acknowledge that you have read this disclaimer
and agree to
all of its terms. Before making any decisions regarding your health or if you have any medical questions, you
should first consult a physician or qualified health care professional who can provide recommendations tailored
to your specific needs. The information published on this site does not constitute a recommendation for
treatment (preventive or curative), a prescription or a diagnosis and is not a substitute for the advice of a
physician or qualified health professional.
As medical and technical knowledge is constantly evolving, the content of this site is made available for
information purposes only. The contributors to this site, including clinical experts in pediatrics from across
Quebec, make every effort to ensure that the information made available on this site is as accurate and reliable
as possible, without guaranteeing the completeness or total absence of error of its content. The opinions
contained in this site are the sole responsibility of the author(s) and are not binding on the contributors to
this site. These opinions do not necessarily reflect the official viewpoint of the organizations mentioned, nor
that of their directors or representatives. The contributors to this site cannot and will not assume any
responsibility for the use of the published content or for the information otherwise accessible through any link
or reference source. Any quotation or reference to a source external to this site is for informational purposes
only and does not constitute an endorsement or claim, express or implied, regarding the content or validity of
the information obtained from that external source.
All rights reserved: The contents of this site may not be reproduced or disseminated, in whole
or in part, in any manner or by any means, electronic, mechanical, including photocopying, recording, or
otherwise, or stored in a retrieval system of any kind that is not limited to private use, without the prior
written permission of the copyright holder.
 Contains glucose in concentrations of 0.5%, 1.5%, 2.5% or 4.25%, sodium, calcium, magnesium, chloride and lactate.
Contains glucose in concentrations of 0.5%, 1.5%, 2.5% or 4.25%, sodium, calcium, magnesium, chloride and lactate.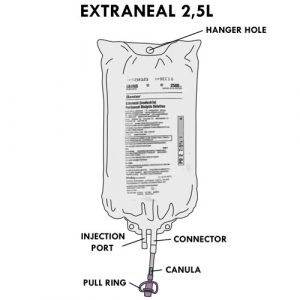

 Cassette: has two separate compartments; one is used to measure the amount of dialysate infused and the other the amount of effluent drained.
Cassette: has two separate compartments; one is used to measure the amount of dialysate infused and the other the amount of effluent drained.