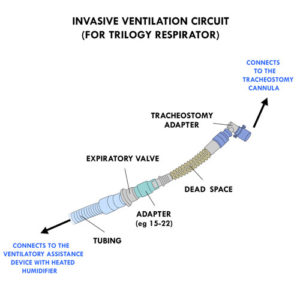
Invasive ventilation provides stable, regular ventilation at a pressure/volume and frequency that is prescribed for your child.
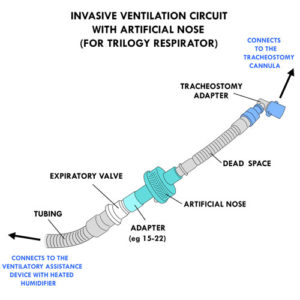
The equipment that is necessary to receive this type of respiratory assistance includes ventilatory assistance device and a ventilation circuit including: tracheostomy adapter, dead space (extension piece of tubing to improve comfort and mobility), adapter (eg, 15-22 mm), exhalation valve (differs according to the different models of ventilatory assistance device) and tubing.
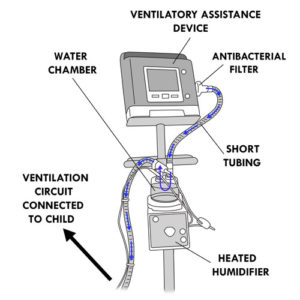
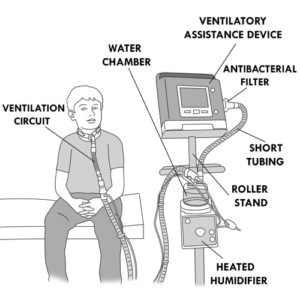
The invasive ventilatory circuit must be connected to a heated humidifier before being connected to a ventilatory assistance device. The heated humidifier warms and humidifies inspired air from the device and is used when the child is stationary.
At the top of the water chamber, there are two openings. One opening of the water chamber is used to connect the ventilatory circuit to the tracheal cannula. Short tubing is connected to the second opening of the water chamber and to the antibacterial filter of the ventilatory assistance device.
The heated humidifier must be removed when the child is mobile or during transportation in order to prevent leaks of water in the ventilatory assistance device or in the circuit.
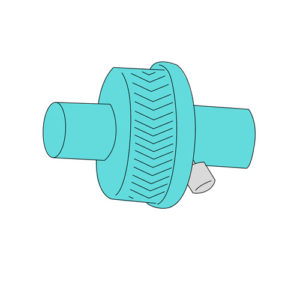
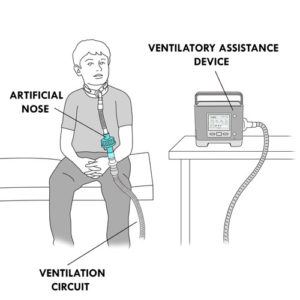
An artificial nose replaces the heated humidifier in an invasive ventilatory circuit when the child is mobile or during transportation.
The artificial nose is inserted between the dead space and the adapter of the invasive ventilation circuit.
There are several different interfaces available to permit non-invasive ventilation.
Non-invasive ventilation with mask provides stable, regular ventilation at a pressure and frequency that is prescribed for your child.
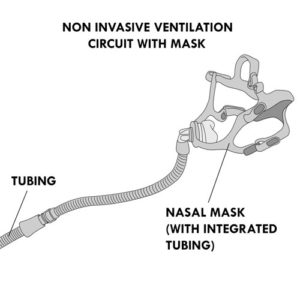
The equipment that is necessary to receive this type of respiratory assistance is a ventilatory assistance device and a ventilation circuit which includes a mask (nasal, facial or nasal pillows) with integrated tubing.
All masks have an exhalation valve (or escape valve) for expiration of exhaled carbon dioxide gas.
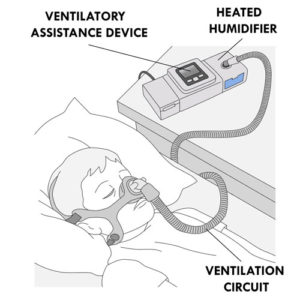
The non-invasive ventilation circuit with mask must be connected to a heated humidifier before being connected to a ventilatory assistance device. The heated humidifier warms and humidifies inspired air from the device and is used when the child is stationary. The heated humidifier must be removed when the child is mobile or during transportation in order to prevent leaks of water in the ventilatory assistance device or in the circuit.
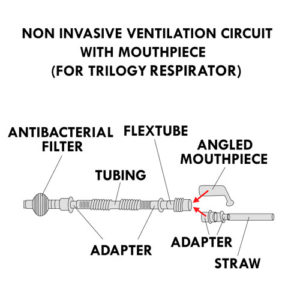
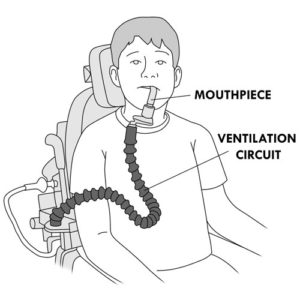
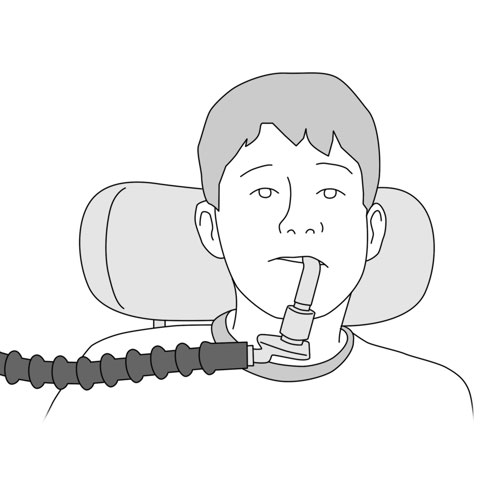
Non-invasive ventilation with mouthpiece is an “as needed” type of ventilation where the child initiates use of the interface to breath in (inspiration) when desired. An expiration device is not required as the child breathes out independently.
This type of ventilatory assistance is used for children who can identify their own breathing needs and who are capable of putting on the mouthpiece and initiating a breath.
The equipment that is necessary to receive non-invasive ventilation with mouthpiece includes ventilatory assistance device and a ventilation circuit which includes a mouthpiece, adapters and tubing.
Non-invasive ventilation with mouthpiece is used only during the day, when the child is awake; at night, or during sleep, these children would use non-invasive ventilation with a mask.
Your healthcare team will recommend the appropriate interface for your child (including headstraps, if required) which will best meet your child’s non-invasive ventilatory needs and adapts to the child’s daily activities. The interfaces are available in a variety of models and formats.
INTERFACES FOR NON-INVASIVE VENTILATION
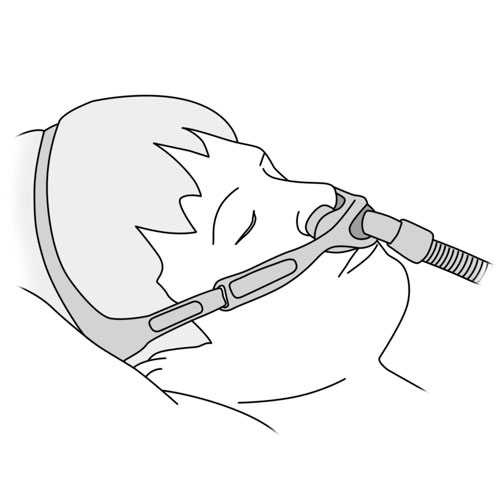
Nasal mask
Covers only the nose.
First choice of interface for infants.
Covers a smaller area than a facial mask and so reduces risk of air leaks.
Easier to adjust fit in a child.
Each mask has straps to secure the fit around the child’s head.
Some masks come with a short segment of integrated tubing.
Allows the child to communicate more easily because the mouth is not covered.
Facial mask for non-invasive ventilation
Covers the nose and mouth.
ONLY used in children if recommended by the healthcare team.
Includes an anti-asphyxia valve in addition to the exhalation valve. In the event of a power failure or device malfunction, the anti-asphyxial valve allows the child to breathe in fresh air from the room rather than re-breathing exhaled air that is trapped in the mask. However, breathing via a facial mask without ventilatory assistance is for short term use only.
Each mask has straps to secure the fit around the child’s head.
Important to quickly remove the mask if the child is nauseous or vomiting.
May be used with a ventilatory bag to replace a ventilatory assistance device or in an emergency situation.
Not to be confused with other types of facial masks that are used for manual ventilation or cough assist techniques. Those types of masks do not have an exhalation valve.
Nasal pillows (or nasal “seals” or intranasal cushions)
Soft pads (pillows, seals) rest under the nostrils.
May be useful for ventilatory assistance during the day.
Allows the child to communicate more easily because the mouth is not covered.
Prevents obstruction to vision.
Each mask has straps to secure the fit around the child’s head.
Useful in children who develop redness or sores on the nasal bridge.
Not to be used in children who only breathe through their mouth.
May be used with a ventilatory bag to replace a ventilatory assistance device or in an emergency situation.
Mouthpiece (eg, angled mouthpiece, straw)
Plastic mouthpiece shaped like a pipe or straw is placed in the mouth and sealed between the lips or held between the teeth.
The mouthpiece has a flexible support arm which can be attached to wheelchair controls or held in place on another surface.
Allows the child to control the amount of inspired air and the frequency of use; this optimizes the child’s respiration and ability to cough while allowing for verbal communication.
Supports inspiration but must be removed from the mouth in order for the child to exhale.
The type of ventilatory assistance device connected to the interface varies depending upon the needs and characteristics of the child (eg, ventilatory needs, weight of the child).
VENTILATORY ASSISTANCE DEVICE
Bi-level (eg, BiPAP®, VPAP®)
Provides two different pressure levels: inspiratory phase pressure (called “IPAP“) and a lower pressure expiratory phase pressure (called “EPAP“). When the child takes a breath, the device senses the effort and pushes more air and increases the pressure up to the IPAP level. At the end of inspiration, the device automatically switches to the expiration phase. The air pressure is decreased until the EPAP level is reached, allowing the child to exhale comfortably.
In addition to supporting the natural breathing of the child, the device has the ability to also initiate breathing (inspiration/expiration) in order to maintain a pre-set minimal number of breaths/minute, thus ensuring adequate ventilatory assistance.
The IPAP, EPAP, and rate of breaths are set by the healthcare team and adjusted to the specific needs of the child.
This device is mainly used for non-invasive ventilation with facial mask, nasal mask or nasal pillows.
Each bi-level ventilatory assistance device is equipped with a removable heated humidifier.
Several models are currently available on the market.
Respirator (eg, Trilogy, Astral)
Provides a specific air pressure (called “controlled pressure“) or a precise amount of air (called “controlled volume“).
Provides two different pressure levels: inspiratory phase pressure (called “IPAP“) and a lower pressure expiratory phase pressure (called “EPAP“). When the child takes a breath, the device senses the effort and pushes more air and increases the pressure up to the IPAP level. At the end of inspiration, the device automatically switches to the expiration phase. The air pressure is decreased until the EPAP level is reached, allowing the child to exhale comfortably.
All the parameters for IPAP, EPAP, frequency, volume and pressure are set by the healthcare team and are adjusted to the specific needs of the child.
Device is mainly used for invasive ventilation or non-invasive ventilation with mouthpiece.
May be used for non-invasive ventilation requiring settings that are not available on the bi-level devices.
May be used with several types of masks (facial, nasal or nasal pillows).
Should be used with a heated external humidifier for invasive or non-invasive ventilation with mask, when the child is stationary. When the child is mobile or during transportation, should be used with an artificial nose in replacement of a heated external humidifier in order to prevent leaks of water in the respirator or in the circuit.
An antibacterial filter should be installed at the ventilatory air outlet during ventilatory assistance.
Each ventilatory assistance device is equipped with visual and audible alarms to indicate if there is a technical problem (eg, too many air leaks in the circuit, device failure, loss of power supply) or related to a change in the condition of the child (eg, accumulation of secretions, respiratory deterioration, excessive or inadequate pressure or volume of air). Refer to your healthcare team or the device instruction manual for further details.
A T-piece can be added to the invasive and non-invasive ventilation circuit of certain devices to allow inhalation of an aerosol medication contained in a small volume nebulizer. Refer to your healthcare team for the specifics of administration technique.
Air leaks can occur during invasive or non-invasive ventilation. They may occur for various reasons, including when: tubing is poorly connected, the mask is poorly fitted to the face or the child is inadequately positioned during sleep. If air leaks are not well controlled, then the effectiveness of the invasive or non-invasive ventilation is not optimal. Air leaks can also cause eye irritation in children who use non-invasive ventilation.
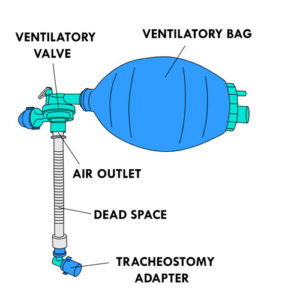
Manual ventilation is provided using a ventilatory bag.
This device consists of a bag and a ventilatory valve to provide an inspiratory volume of air to an individual who is unable to breathe in sufficiently. This device also allows for the elimination of carbon dioxide. The ventilatory bag can replace a ventilatory assistance device in the event of an emergency or power failure.
Different ventilatory bag models are available, depending upon the amount of air delivered by compression. The amount of air delivered corresponds to the depth of compression.
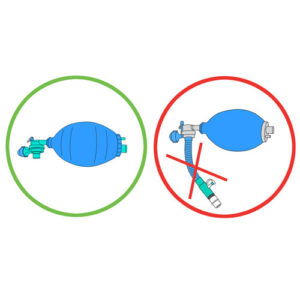
Do not confuse the ventilatory bag for manual ventilation with the modified ventilatory bag which is a specific device used for cough assistance techniques. The modified ventilatory bag does not allow the child to exhale which is DANGEROUS.
The air outlet of the ventilatory bag is connected to a tracheal cannula or a facial mask specific to this use.
If necessary, the air outlet of the bag can be connected to a dead space and a adapter before being connected to the tracheal cannula.
A ventilatory bag may also be used with a tracheostomy adapter.
The facial mask used for manual ventilation does not have an exhalation valve or straps to fit around the child’s head.
Your healthcare team will determine whether your child requires a manual ventilatory bag and/or a second ventilatory assistance device as a back-up in the case of an emergency.
Disclaimer of Liability: By using this site, you acknowledge that you have read this disclaimer
and agree to
all of its terms. Before making any decisions regarding your health or if you have any medical questions, you
should first consult a physician or qualified health care professional who can provide recommendations tailored
to your specific needs. The information published on this site does not constitute a recommendation for
treatment (preventive or curative), a prescription or a diagnosis and is not a substitute for the advice of a
physician or qualified health professional.
As medical and technical knowledge is constantly evolving, the content of this site is made available for
information purposes only. The contributors to this site, including clinical experts in pediatrics from across
Quebec, make every effort to ensure that the information made available on this site is as accurate and reliable
as possible, without guaranteeing the completeness or total absence of error of its content. The opinions
contained in this site are the sole responsibility of the author(s) and are not binding on the contributors to
this site. These opinions do not necessarily reflect the official viewpoint of the organizations mentioned, nor
that of their directors or representatives. The contributors to this site cannot and will not assume any
responsibility for the use of the published content or for the information otherwise accessible through any link
or reference source. Any quotation or reference to a source external to this site is for informational purposes
only and does not constitute an endorsement or claim, express or implied, regarding the content or validity of
the information obtained from that external source.
All rights reserved: The contents of this site may not be reproduced or disseminated, in whole
or in part, in any manner or by any means, electronic, mechanical, including photocopying, recording, or
otherwise, or stored in a retrieval system of any kind that is not limited to private use, without the prior
written permission of the copyright holder.